
A study presented at the American College of Cardiology Annual Scientific Session, known as the PRO-TAVI trial, reported that elderly patients suffering from coronary artery disease who were scheduled for Transcatheter Aortic Valve Replacement (TAVR) experienced similar clinical outcomes whether they underwent Percutaneous Coronary Intervention (PCI) before the valve procedure or postponed it until later.
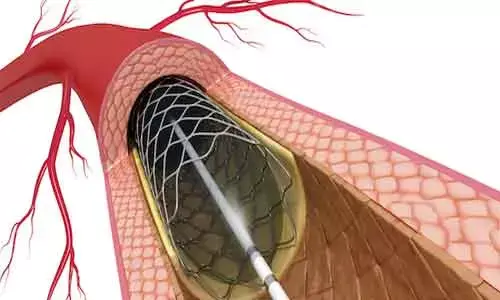
TAVR is a minimally invasive technique used to treat a narrowed aortic valve. During the procedure, doctors insert a new valve through a catheter—most often through the femoral artery in the groin—and position it inside the damaged valve. PCI, commonly referred to as angioplasty, is another catheter-based procedure in which a stent is placed through an artery (often the radial artery in the wrist or arm) to open blocked coronary arteries and restore blood circulation to the heart.
For individuals who have both severe aortic valve disease and coronary artery blockages, the ideal sequence and combination of these two procedures has long been uncertain. Treatment strategies differ across regions. In many European countries, where TAVR is primarily performed on older or high-risk patients, cardiologists often delay PCI until after TAVR. In contrast, physicians in the United States frequently recommend performing PCI before the valve replacement because TAVR candidates tend to be younger and in better overall health.
The clinical trial was conducted in the Netherlands and its results support the practice commonly followed there. Physicians in the region usually avoid performing PCI before TAVR unless there is a strong medical indication. The findings revealed that skipping PCI before TAVR did not increase the likelihood of serious complications such as death, heart attack, stroke, or significant bleeding.
According to Michiel Voskuil, an interventional cardiologist and professor at University Medical Center Utrecht and the study’s lead researcher, it may be reasonable to perform TAVR first in elderly patients with coronary artery disease. If symptoms like chest pain or pressure persist after the valve procedure, PCI can then be performed later if required.
The trial involved 466 participants treated at 12 medical centers across the Netherlands between 2021 and 2024. The median age of patients was above 80 years, and about 36% were women. All patients had significant coronary artery blockages and represented a high-risk group typically seen in European TAVR programs.
Participants were randomly divided into two groups. One group underwent PCI before receiving TAVR, while the other group had TAVR first and only received PCI afterward if symptoms continued or worsened.
Researchers assessed a combined primary outcome that included death from any cause, heart attack, stroke, or moderate to severe bleeding within 12 months. This outcome occurred in 25.8% of patients who had PCI before TAVR and in 24.1% of those who postponed PCI. The difference fell within the study’s predefined non-inferiority margin, indicating that both strategies produced similar overall results.
However, the groups differed when it came to major bleeding events. About 14.8% of patients who underwent PCI before TAVR experienced significant bleeding, compared with only 6.2% of those who delayed PCI. Investigators suggested that the higher bleeding rate might be related to the dual antiplatelet medications commonly prescribed after PCI, particularly since many bleeding events occurred around the time of the TAVR procedure. Despite this increase, there was no additional risk of death linked to these bleeding episodes.
In total, approximately 10% of patients who initially postponed PCI eventually required the procedure because of ongoing or worsening symptoms after TAVR.
Researchers emphasized that the findings mainly apply to European healthcare settings—especially the Netherlands—where TAVR is largely performed in older, higher-risk patients. The results may not directly apply to regions where younger and healthier individuals commonly undergo TAVR.
Voskuil noted that the trial focused specifically on intermediate- and high-risk patients. For lower-risk individuals, who are generally younger, the best treatment approach remains uncertain and further clinical studies may be needed to determine the most effective strategy.





